


Specialty Drug Costs Are No Laughing Matter for Employers
We’ve all heard the commercials. The lengthy list of possible side effects and potential complications makes us laugh and question whether taking the medication will make you sicker than the disease it’s trying to treat. What’s not funny, especially to employers, is the cost of these wonder drugs, called “specialty drugs” in pharma and benefits parlance.
Specialty drugs are special in the sense that they’re complex medications developed to treat complex or chronic conditions like rheumatoid arthritis, heart failure and cancer. They’re also special because of their price. Medicare defines a specialty drug as one that costs at least $670 for a 30-day supply.
As you know from reading the papers (that’s newspapers, if you don’t remember), many new specialty drugs cost more than $10,000 per month. A recent example is a new drug that goes by the brand name Kymriah, which was approved by the FDA in August (bit.ly/2grlPdB). It’s an immunotherapy drug that’s customized with the patient’s own genetic material to treat leukemia in children and young adults. The list price for one course of treatment, which takes less than an hour to administer after the manufacturer takes up to four weeks to mix the custom brew, is $475,000, per Reuters (that’s a news service).
Curing your teenage son or daughter of cancer is priceless. But for those who have to pay most of the bill, namely employers, it’s another call to action to do something to control specialty drug costs, lest they break the employee health benefits bank.
Some numbers from the QuintilesIMS Institute tell the story. In 2007, the net per-capita spending on prescription medications in the U.S. was $811, with 24 percent spent on specialty drugs. By 2016, the net per-capita spending on prescription medications in the U.S. rose 10.4 percent, to $895, but 43 percent was now spent on specialty drugs (bit.ly/2tUzmN8).
A number of recent employee benefits surveys reveal how employers feel about that trend and how they intend to address it. Managing specialty drug costs was the top priority of nearly 300 employers recently surveyed by the Pharmacy Benefit Management Institute (bit.ly/2j4VnZ3). Making sure workers taking specialty drugs were satisfied was far less important to management (see chart).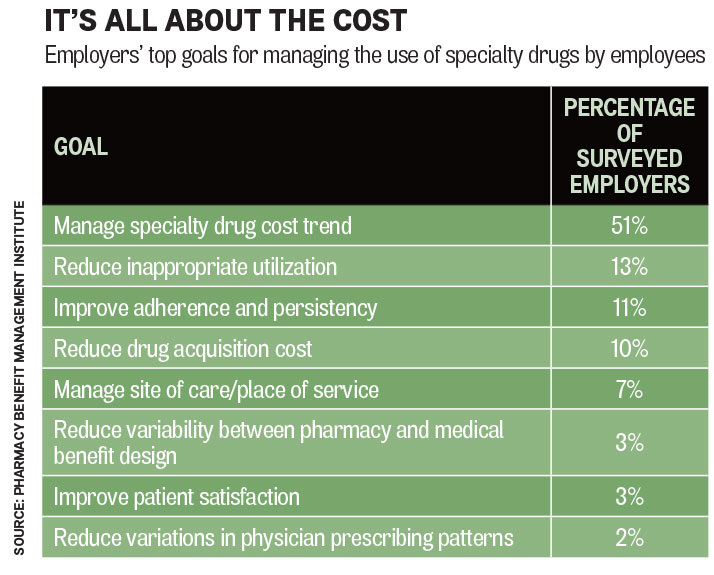
By far the top driver of rising employee health care costs is specialty drugs, according to a 2017 survey of 148 large employers by the National Business Group on Health (bit.ly/2vMp3yW). Some 80 percent of the employers cited specialty drugs as one of three top drivers of health spending. That was followed by high-cost claimants (69 percent) and specific diseases or conditions (55 percent). High-cost claimants often have specific diseases or medical conditions that require specialty drugs.
Asked what they were going to do about it in 2018, the employers most frequently cited these tactics, in order of rank:
Read more from this issue
- Adopting more aggressive utilization management protocols (71 percent)
- Requiring specialty drugs to be obtained through a specialty pharmacy or specialty department of a pharmacy benefits manager (68 percent)
- Managing the site of care where the drugs are administered (44 percent)
- Including a specialty drug tier in pharmacy benefit design (38 percent)
- Requiring prior authorization for specialty drugs covered as a medical benefit (31 percent)
- Using high-touch case management (30 percent)
Another tactic being used by employers is requiring workers who use specialty drugs to pick up a larger share of the tab. A 2017 survey of more than 2,100 employers by the Kaiser Family Foundation and the Health Research & Education Trust found that 97 percent of employers offer specialty drug coverage, with 47 percent including a specific specialty drug tier in the benefit design (kaiserf.am/2fcLdzS).
The average co-payment for a medication covered in the specialty drug tier was $101 last year, with the average co-insurance share 27 percent. By comparison, the average co-payment for a medication covered in the first tier of a pharmacy benefits package was $11 last year, with an average co-insurance rate of 17 percent.
If all else fails, employers can lobby the FDA, the Federal Communications Commission and the Federal Trade Commission to restrict direct-to-consumer advertising of high-cost specialty drugs by Big Pharma. Some 90 percent of employers surveyed by the PBMI said DTC advertising “greatly” or “moderately” increases the pressure on physicians to prescribe a specific specialty drug. Another 76 percent said it increases the number of patients seeking medications for previously undiagnosed medical conditions.
If laughter is the best medicine, though, keep the DTC advertising and I’ll take my chances.
Short Take
Speaking of arthritis, I don’t have it yet from writing this column. But if and when it does happen, it will cost you big—or, more specifically, it will cost my employer. A new study pegged the total national cost incurred by working adults with arthritis at $303.5 billion in 2013 (bit.ly/2AmniLu ). The study, from the Division of Population Health at the Centers for Disease Control and Prevention, appeared in the journal Arthritis Care & Research, appropriately enough. Of that amount, $139.8 billion was spent on medical services. Even more—$163.7 billion—came from earning losses of those whose arthritis prevented them from doing their job. Maybe there’s a return on investment in specialty drugs for employers after all.
David Burda (twitter.com/@davidrburda; dburda@msp-c.com) is editorial director, health care strategies, for MSP-C, where he serves as the chief health care content strategist and health care subject matter expert.



