


The Workforce’s Hidden Addicts
Steve Rummler of Eden Prairie was not a high-profile CEO or business leader. He was an independent financial planner who worked through the network of Minneapolis-based AdvisorNet Financial. Like many others in the local business community, he held a degree in economics from the University of Minnesota. His death in 2011, at the age of 43, did not make headlines.
Doctors originally prescribed opioid painkiller Oxycontin in 2005 for Rummler’s chronic back pain, but his use of the drugs steadily increased. Rummler tried to get off them. He went through treatment, but relapsed. When he could no longer find a way to get a prescription for the painkillers, he tried switching to heroin. He overdosed and died in July 2011.
After his death, his family created Minnetonka-based Steve Rummler Hope Network to raise awareness about addiction issues for people grappling with chronic pain.
“I frankly am very concerned for our country because the economic cost is so much greater than what people are looking at,” says Lexi Reed Holtum, who was Rummler’s fiancée and now serves as the organization’s executive director.
But it’s extremely difficult to calculate the total cost of prescription opioid abuse, she says, because it includes significant ripple effects beyond loss of business clients or workplace disruption; it affects family members, friends and others in an addict’s circle. For example, after Rummler died, Holtum took a full month off from work.
The number of opioid deaths in Minnesota is not as alarming as in many other states, but it keeps climbing. Total Minnesota drug overdose deaths were up from 129 in 2000 to 572 in 2015. Deaths due to opioid pain relievers over the same period rose from 23 in 2000 to 216 in 2015. Heroin deaths went from just 2 in 2000 to 114 in 2015. Middle-aged people were at the greatest risk: From 2013 to 2015, a total of 411 Minnesotans ages 45 to 54 died of drug overdoses, or 25 percent of all overdoses in the state in that period.
New Jersey-based Quest Diagnostics Inc., which offers drug testing across the U.S., reported in May that the rate of positive drug tests among workers hit its highest level in 12 years in 2016. Quest found that nationwide, workers tested positive at a rate of 4.2 percent; Minnesota came in at 3 percent. Many employers do not screen for prescription opioids; in Minnesota less than 10 percent of employers who do drug testing are screening for prescription opioids.
Fortune 500 electronics retailer Best Buy Co. recently became the Rummler foundation’s first corporate partner, training and certifying its security staff to administer Naloxone, an emergency treatment for opioid overdose.
Best Buy took the action after an incident in late 2016, when a car pulled up in the traffic circle of its Richfield headquarters with a passenger (not a Best Buy employee) in the middle of a drug overdose. Given the large number of people who work at Best Buy’s corporate campus—about 5,000 people including other tenants—the company’s security staff thought it an important step to take.
Best Buy spotlighted the initiative in early August. “While we hope we never need to put this Naloxone training to use, we wanted to ensure we have the training and equipment necessary to render proper aid to a person in distress,” said Kellen McWhite, Best Buy’s senior manager of crisis management and security, in a blog post on the corporate website.
Asked about Best Buy’s efforts, spokesman Jeff Shelman declined comment. He’s not alone—several companies contacted for this story have little to say on the subject. In most cases, it’s because they say they simply aren’t seeing it.
Still hidden here
“Nobody here is going into the emergency room, and we’re not taking anyone home because of it. Every once in a while we have someone who shows up drunk, but nothing with [opioids],” says Reggie Clow, CEO of Merrifield-based Clow Stamping Co. in the Brainerd area. The company employs about 450 people. “We hear about it and meth in the papers, and meth is probably a bigger thing up here, but we’re not seeing it at work.”
Many other business and industry leaders, including six major manufacturers in northern Minnesota, say that they haven’t seen any widespread indications of a problem.
The issue also does not appear to be of concern in the building and construction sector. “The good majority of building trades unions and owners that we work for typically have some form of pre-employment drug screening,” says Harry Melander, president of the Minnesota State Building & Construction Trades Council. “For the most part, we feel fairly fortunate that it hasn’t become a huge issue for our industry. It’s an issue that we’ve discussed, but it isn’t one that’s started to burn a hole in our workforce as of yet.”
One reason it’s apparently not showing up could be because symptoms of opioid addiction are not as obvious as are those of other drugs subject to abuse, such as alcohol. Rather than stumbling or slurred speech, an opioid addict might just seem overly tired. They’re also often fairly functional; treatment professionals estimate three out of four people abusing prescription opioids are employed.
Read more from this issue
“The person might be a little sedated on those medications,” says Dr. Charles Reznikoff, an addiction medicine doctor with Hennepin County Medical Center. “Addicts can function on a day-to-day basis surprisingly well.” But as their addiction worsens, signs start to show (see “Warning Signs,”).
Another reason could be that it just isn’t as big a problem here yet. But it is elsewhere in the country, prompting experts to say it’s only a matter of time until it becomes more obvious in Minnesota businesses. In its 2015 National Survey on Drug Use and Health, the federal Substance Abuse and Mental Health Services Administration estimated that 3.8 million Americans age 12 and older were misusing pain relievers.
Indeed, there are some signs that may be starting to happen.
A June report from the Cambridge, Mass.-based Workers Compensation Research Institute found that 78 percent of Minnesota employees who filed a worker’s comp claim from 2013 to 2015 and were prescribed a painkiller were prescribed at least one opioid. (The study looked at non-surgical cases with more than seven days of missed work.)
A recent report from the Centers for Disease Control and Prevention (CDC) found that the risk for addiction increases exponentially with time. An individual who used an opioid for just one day had a 6 percent probability of using opioids a year later. Of those prescribed an opioid for eight days or more, 13.5 percent were still on them a year later. When the initial prescription lasted 31 days or more, 30 percent were still taking them a year later. Meanwhile, the cost of prescription opioids is going up, while illegal opioids and heroin are getting cheaper (and easier to obtain).
There are some encouraging signals that opioid awareness campaigns are starting to show an impact. A July report from the CDC found that the total amount of opioids prescribed dropped 18 percent from 2012 to 2015. But the CDC noted that the number of opioid prescriptions in 2015 was still triple the amount in 1999.
One former high-flying sales executive turned treatment professional calls individuals who fall into this trap “accidental addicts”—people who never planned to use hard drugs, but were initially prescribed opiates after surgery or, most commonly, to deal with back pain. “Then, like any addiction, once you’re in it, you’re in it,” says Bob Poznanovich, executive director of business development for Center City-based Hazelden Betty Ford Foundation.
Meanwhile, the huge proliferation of opioid prescriptions is fairly recent, reaching a record 240 million in 2014, the most recent year that figures were available, according to UnitedHealth Group. This is up from 155 million in 2004 and does not include an equally recent increase in the availability of opioids from non-legal sources—primarily fentanyl (the drug that caused Prince’s death), which is 50-times more powerful than heroin and easily available without a prescription through the Dark Web.
Opioid deaths have been climbing since the late 1990s, though Hans Hage, vice president of product development for Eagan-based StayWell, says that he began noticing more reports of opioid concerns within the last two years, first noticing it among heavy-manufacturing employees and other shift workers. “Now it’s like every client I go into, it comes up—really, any industry.” StayWell provides wellness programs for client companies.
“There’s all the employee assistance programs that are out there that originally started around alcoholism . . . the opioid issue is the one that’s the most lethal bullet out there right now,” says Dr. Steve Lansing, CEO and clinical director of Rochester-based EmPower Comprehensive Treatment Center. “We’ve had businesses that have lost people to overdoses.”
Lansing says that EmPower is developing an educational program for employers about the issue. “The need is so significant,” he says. “There’s still a lot of ignorance out there and misinformation.” He adds that many business owners in Minnesota are wary of discussing the costs and challenges of employees addicted to prescription opioids. “They don’t want their business to look like a problem.”
Other treatment professionals agree that companies grappling with the issue are doing so behind the scenes and don’t see any upside to talking about the issue publicly.
“Employers aren’t sharing this issue with each other . . . they’re going to their health care providers and saying ‘Help us solve this,’ ” says Pablo McCabe, director of national strategic accounts for Hazelden Betty Ford Foundation, the nation’s largest nonprofit treatment provider. “People are trying to manage it quietly on their own . . . but numbers don’t lie.”
Nationally, CDC statistics show that prescription opioid deaths have more than quadrupled since 1999. In 1999 the CDC tallied 3,442 deaths. By 2015, prescription opioid deaths had climbed to 15,281, roughly 42 deaths per day. Between 2000 and 2015, a total of 5,709 Minnesotans died from drug overdoses; 2,273 of them died due to opioids.
Meanwhile, more and more companies are forced to deal with the issue—but don’t know how. V. John Ella, with the Minneapolis-based Trepanier MacGillis Battina law firm, says he’s increasingly hearing concerns about opioids from businesses. “They say, ‘We think this guy’s on painkillers, and what do we do about it?’ ” says Ella, who represents companies on a range of issues, including drug testing.
“There’s an uptick,” he says. “It’s not something that companies really pay attention to until they start to get into the soup.”
Measuring the impact
In July, Federal Reserve Chair Janet Yellen said she believes that the opioid crisis was related to “declining labor force participation among prime-age workers.”
In its Beige Book released in July, the St. Louis Federal Reserve reported: “Manufacturing contacts in Louisville and Memphis reported difficulties finding experienced or qualified employees, with some citing candidates’ inability to pass drug tests.”
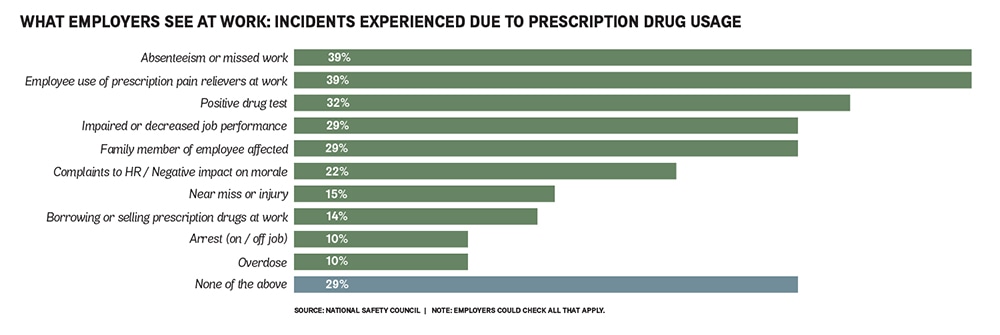
A March study of companies across the U.S. with 50 or more employees found that 71 percent of employers reported being affected by prescription drug use by employees. It was conducted by the National Safety Council (NSC) in conjunction with the University of Chicago and nonprofit Shatterproof.
Employers cited absenteeism or workers with impaired or decreased job performance as top issues, the survey found. Its findings also revealed 22 percent of employers reported complaints to the human resources department or a “negative impact on employee morale” as concerns; 14 percent cited concerns about employees “borrowing or selling prescription drugs at work.”
Among other findings from the study, How the Prescription Drug Crisis is Impacting American Employers:
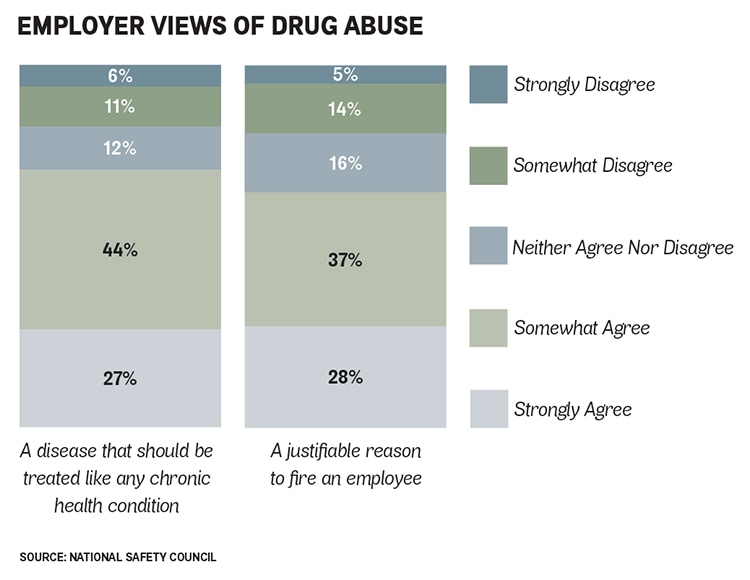
- 71 percent of employers agree that prescription drug misuse is a disease that requires treatment.
- 65 percent feel it is a justifiable reason to fire an employee.
- 88 percent are interested in their insurer covering alternatives to pain-relief treatment so that employees can avoid taking opioids.
Similarly, a 2016 study of 200 Indiana employers conducted by the National Safety Council and the Indiana Attorney General’s Prescription Drug Abuse Prevention Task Force reported that prescription drug abuse currently affects 80 percent of companies.
Meanwhile, there are the costs.
Human resources, legal and treatment experts say that opioids are the reason for increasing health care costs, an uptick in absenteeism, a drain on productivity and rising turnover. National studies estimate annual costs to employers in the range of $18 billion to $25.6 billion.
Based on the percentage of total U.S. jobs in Minnesota, a rough estimate would put the state’s costs at 2 percent— ranging from $360 million to $512 million—of the national total.
For individual employers, a 2014 study from the Boston-based Analysis Group Inc. found annual health care costs of $20,343 for employees abusing opioids, compared with $9,716 for non-addicted employees.
The NSC now offers a “substance use cost calculator” for employers, based on state, industry and total number of employees (and factoring in all drugs, including alcohol, not just opioids). Entering a hypothetical Minnesota durable goods manufacturing company with 500 employees into the calculator yields an estimated annual cost of about $170,000 due to health care expenses, lost time on the job and costs related to employee turnover and retraining.
And as Reed Holtum pointed out earlier, there are ripple-effect costs.
The CDC estimated the overall societal cost of prescription opioids at $78.5 billion for 2013. Dr. Curtis Florence, lead health economist for the CDC’s National Center for Injury Prevention and Control, estimates that 65 percent of those costs were borne by companies and employees (the CDC did not calculate a standalone estimate for costs to businesses). Florence says that increased health care costs, criminal justice costs and lost productivity are the largest categories making up total cost.
The steep price of the opioid problem was not unexpected. “I don’t think we were surprised. We were concerned with the magnitude of this problem,” says Florence. “We did this to show what kind of costs could be avoided.”
And in the big picture, prescription opioids are not the nation’s biggest substance abuse threat. The CDC’s report contrasted the estimated opioid costs with estimated costs for tobacco ($300 billion, 2010), alcohol ($249 billion, 2010) and illicit drugs ($193 billion).,/p>
 No one is immune
No one is immune
The opioid crisis underscores what treatment professionals know: Addiction can afflict anyone. That includes people with high-paying white-collar jobs such as attorneys.
Lawyers and law firms historically have not been wired to ask for help, says Patrick Krill, an attorney who leads the St. Paul-based Krill Strategies, which works with mid-size to large legal firms nationwide. “The legal profession is especially competitive. They’re supposed to be the people solving the problems.”
In many cases, Krill sees senior management of a law firm spending “countless hours” in closed-door meetings trying to figure out how to handle a lawyer who appears to be having trouble due to substance abuse. That’s another cost to businesses, he says, and “one thing that I think is really underreported.”
Beyond an uptick in opioids, Krill sees modern work culture as a factor in overall substance abuse. “People are more burned out, more anxious, more depressed than ever before. The demands of the workplace are changing. […] I think generally professions are more competitive and less secure. What I see with lawyers is the expectation of around-the-clock availability.”
Wisconsin-based nonprofit MRA–The Management Association provides human resources support and services for member companies. The group operates an “HR hot line” that members with problems can call 24 hours a day. Employers are increasingly asking how to navigate workplace addiction issues, according to Laurie Greenlees, who manages the hot line. MRA serves about 950 organizations, with 370,000 employees in Minnesota.
“The most common question that we’re fielding is employers working through situations where they have an employee whom they believe is under the influence at work,” she says. “With the opioid epidemic, I think now is a time when people really should be going back and revisiting their drug testing policies and procedures.”
Such tests need to be updated, too. The Indiana study found that while 84 percent of employers surveyed have drug testing policies, only 52 percent include screens for opioids. In addition, only 53 percent of the employers had policies addressing use of prescription drugs on the job.
There are also the potential legal consequences in testing employees. Many companies are not aware of the details of Minnesota’s drug testing law, which has been on the books since 1987, according to attorney Ella. Under the law, administering a drug test actually gives the employee more legal protection.
It’s not uncommon for a company to fire an employee based on a drug test and then find themselves being sued. While a company can reject a job applicant on the basis of a drug test result, Ella says a business cannot legally fire an employee on the basis of an initial positive test result once he or she is employed.
“The core of the law in Minnesota is if you test an employee for drugs and alcohol, you can’t terminate them . . . unless you’ve given them a chance to go to treatment and they either refuse or fail to complete it,” says Ella.
Ella adds that employers need to have clear, explicit policies on drug issues, spelling out the rules and consequences to employees.
Others recommend that, instead of firing an individual, he or she should be directed to an employee assistance program that ensures employees with any type of substance abuse problem can get treatment, rehabilitation and support, so they can successfully return to work.
On a larger scale, the Steve Rummler Hope Network organized an “Opioid Awareness Day” at the Minnesota Capitol in February to draw more attention to the issue. During the legislative session, the foundation was backing a bill to create a state opioid stewardship program, which would have included efforts to boost education, prevention and treatment. The proposal would have raised an estimated $21 million annually through a fee levied on pharmaceutical manufacturers that sell opioids in the state. Two business groups, the Minnesota Chamber of Commerce and Medical Alley Association, opposed the bill and testified against it. The bill did not pass.
Authors of the bipartisan effort included Sen. Julie Rosen, who defines herself as a “conservative Republican.” If the ongoing opioid crisis is a wake-up call for the state, Rosen says that the legislature is not answering the phone:
“It certainly does have an impact on businesses, and it’s everybody’s problem. And I don’t see anything in the state to date that makes me think we’re getting our hands around this. I think everybody recognizes it’s a problem. I don’t see any movement to make it a priority yet.”
What is an Opioid?
There’s a common misperception that an opioid is something reserved for special cases, but it’s not. Drugs such as heroin, morphine and codeine are opiates and commonly associated with street junkies. The term “opioid” was coined to describe versions of opiates that could be produced by pharmaceutical companies, legally distributed as painkillers, and taken as pills. They include fentanyl, hydrocodone, oxycodone, OxyContin, Percocet and Vicodin. More than one-third of Americans were prescribed an opioid in 2015, according to a National Survey on Drug Use and Health released earlier this year.
How Much Does Opioid Abuse Cost, Really?
The truth is no one knows exactly how much opioid abuse is costing employers in increased absenteeism, rising health care costs, reduced productivity and other factors. Media reports cite varying numbers, in some cases from studies that are several years old.
There are no reports for employers in Minnesota. Based on statistics for June, Minnesota accounted for approximately 2 percent of all U.S. jobs. A rough estimate would put the state’s costs to employers at 2 percent of the total estimated costs for U.S. employers.
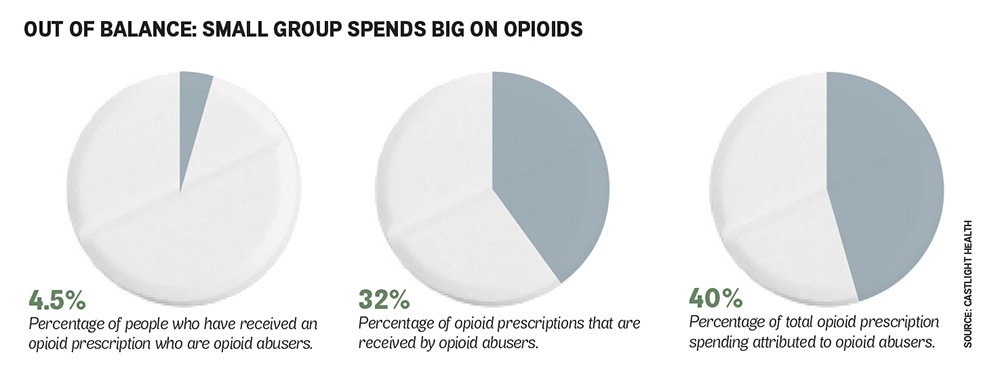
- An April 2016 report from San Francisco-based Castlight Health estimated annual employers’ costs of opioid abuse at $18 billion—up to $8 billion in increased health care costs plus another $10 billion in absenteeism and presenteeism. “This crisis represents a significant drain on America’s employers,” the study noted.
- In 2016, CDC researchers calculated the total cost of prescription opioids in the United States at $78.5 billion, including $26 billion in increased health care costs. CDC researchers did not break out an estimate of the cost to U.S. companies.
- An oft-cited 2011 study in the Pain Medicine journal estimated workplace costs of prescription opioid abuse at $25.6 billion in 2007, nearly half of the then-estimated societal costs of $55.7 billion.
Issues for Employers
Many employers find themselves unprepared to appropriately deal with an employee who may be battling a prescription opioid addiction. Here are a few questions that owners, managers and human resource staff should be asking:
- Do managers know warning signs of an employee who is under the influence of opioid painkillers?
- Does the company have a clearly outlined and updated drug policy?
- Does the company regularly communicate with employees to ensure that they are aware of policies and expectations?
- Does the company culture make employees feel comfortable reporting concerns about co-workers to management?
- Is the company in compliance with Minnesota’s drug testing law (and its own policies)?
- If the company drug-tests employees, does the test screen for prescription opioids?
- What treatment options are covered under the company’s health care plan?
Warning Signs
Most opiate abusers with costly habits are not readily identifiable as addicts, especially at first. They come from nearly every walk of life, and many have good jobs. But as their addictions progress, their urge to find their next “high” begins to interfere with other aspects of their lives.
Opioid addicts tend to be in one of two stages while at work. If they are under the influence of the drugs, at first glance they may seem to be functioning well. However, there may be evidence of mood swings or major changes in energy level. They may appear to nod off while on the job or fall asleep at their workstations, in their cars or even while using the bathroom, according to Safety Management Group, one of the nation’s largest professional safety service companies.
Then, as the effects of the last dose wear off and the craving for the next begins, they may display signs of withdrawal. The symptoms often appear to be the same ones associated with the flu or upset stomachs: sweating, shaking, aches and a runny nose. They may also become irritable and anxious. A worker whose addiction has progressed to injected heroin may need to repeat a dose every few hours, going through the cycle several times a day.
Other warning signs include an unusually high number of pill bottles in trash cans. Addicted employees may develop serious financial problems, requesting advances on pay or trying to borrow money from or sell things to co-workers. It’s not unusual for addicts to withdraw from the social aspects of work, and a once-gregarious worker may suddenly become quiet and sullen.
What’s Being Done in Minnesota?
While there is no Minnesota business group taking a leadership role in the opioid crisis, efforts are underway to raise awareness of the problem and find alternatives for pain management:
- The state established the Opioid Prescribing Work Group in 2015, a group of primarily medical professionals assembling prescribing recommendations on medications for acute pain.
- Attorney General Lori Swanson released a report on the opioid problem in November with a range of policy recommendations. In June, Swanson’s office confirmed that Minnesota is part of a multi-state “ongoing investigation into the potential legal culpability of pharmaceutical manufacturers in the marketing and sale of opioid prescription painkillers.”
- Minnetonka-based UnitedHealth Group, one of the nation’s largest insurers, is implementing policies to prevent opioid abuse. That includes setting a limit on the quantity of opioids that a patient can obtain and using data and analytics to identify patients who may have obtained opioid prescriptions from several doctors.
- Eagan-based Prime Therapeutics, one of the largest pharmacy benefit managers in the U.S., rolled out an updated Controlled Substance Management Program in July. It includes identifying individuals at a higher risk for controlled substance abuse. Company statistics show that its existing programs have already delivered a 16 percent rollback in prescribed opiates over the last five years.
Burl Gilyard is TCB’s senior writer.



