


Hospitals Under Stress
Rahul Koranne will return to the Minnesota State Capitol this month to plead for funding for Minnesota hospitals.
In the world of complex health care finance, Koranne, president and CEO of the Minnesota Hospital Association, wants state lawmakers to patch a hole in the hospital revenue model caused by a logjam of patients.
Koranne, a physician who’s worked for the association for nine years, says it’s exasperating for hospital leaders because they’re often having great difficulty discharging patients.
“We did an analysis of how many patients were stuck in a hospital [who] did not require acute care or a hospital level of care,” he says, referring to research done in late 2022. “There were thousands of patients that were not able to be discharged into a nursing home, a group home, or a mental health care facility.”
“These thousands of patients are literally stuck in the hospital.”
—Rahul Koranne, president and CEO, Minnesota Hospital Association
The patients were well enough to leave the hospital, but they couldn’t go home because they needed to move to another care facility for follow-up treatment or support. But in many cases, patients were forced to remain hospitalized because there wasn’t room for them in care facilities.
Various insurance systems refused to compensate hospitals for this type of care.
“Medicaid doesn’t pay for these patients,” Koranne says. “Medicare doesn’t pay for these patients. Commercial insurance doesn’t pay for these patients. So these thousands of patients are literally stuck in the hospital, the hospital is providing care to these patients, but nobody is paying for the care.”
In 2023, Gov. Tim Walz and the Minnesota Legislature funded a variety of new programs as a result of a budget surplus that exceeded $17 billion. Minnesota hospital leaders were seeking hundreds of millions of dollars to deal with the issue of “uncompensated care.”
“We got only $18 million,” Koranne says, and Minnesota’s Department of Human Services was charged with paying out that money to hospitals. The department sought documentation, and the not-for-profit hospitals produced records for the number of patient care days delivered with no reimbursement for the first five months of 2023.
That $18 million filled just a fraction of the hospitals’ needs, he says. The hospital association extrapolated what the annual need was based on the data from the January-to-May period. “When you do the math, [it was] $450 million.”
Koranne will make another attempt to secure funding in the new session. However, lawmakers will be working with a smaller surplus. In mid-January, Walz indicated that so much legislation was passed in 2023 that the 2024 session likely will have a relatively modest agenda. However, the governor does plan to push hard for a 2024 state infrastructure package. The session opened Feb. 12.
“The state Legislature made a generational investment in our schools and our educational system” in 2023, Koranne says. “We are hoping that in this upcoming legislative session, given that they still have some reserves, that they will make a generational investment in our hospitals, because hospitals are so important for communities.”
He wants funding for what he’s dubbed a rescue package. “It’s going to have to be hundreds of millions of dollars,” he says.
Koranne will be talking to politicians about a new set of financial data, which he released in mid-November. Collected from more than 70 hospitals in the state, the metrics detail a median operating margin of –2.7% for the first half of 2023 compared to –0.5% for the same period in 2022.
Read more from this issue

“We tried to make a loud noise when it dipped into a negative number at a negative half a percent,” Koranne says.
No Minnesota hospitals closed in 2022 or 2023, but several hospitals in other states have shut down in recent years. “That’s the reason for really turning up the volume on this alarm bell,” Koranne says. “We want to try to prevent that [in Minnesota] because it will be too late if a hospital announces a closure.”
In a September 2022 report, the American Hospital Association (AHA) announced that 136 rural hospitals closed in the U.S. between 2010 and 2021. Three factors cited were declining financial performance, geographic isolation, and low patient volumes.
“The bulk of rural hospital revenue comes from government payers, of which Medicare comprises nearly half,” the report says. “Yet both Medicare and Medicaid reimburse less than the cost of providing these services. This resulted in rural hospitals incurring $5.8 billion in Medicare underpayments and $1.2 billion in Medicaid underpayments in 2020.”
Koranne regularly travels around Minnesota to talk with hospital administrators. “We are already seeing reductions in services across the state due to financial strain,” he says. “We are working to pull every lever we can to at least bring government payers closer to being in alignment with the actual costs of providing care.”
Revenue isn’t the only problem
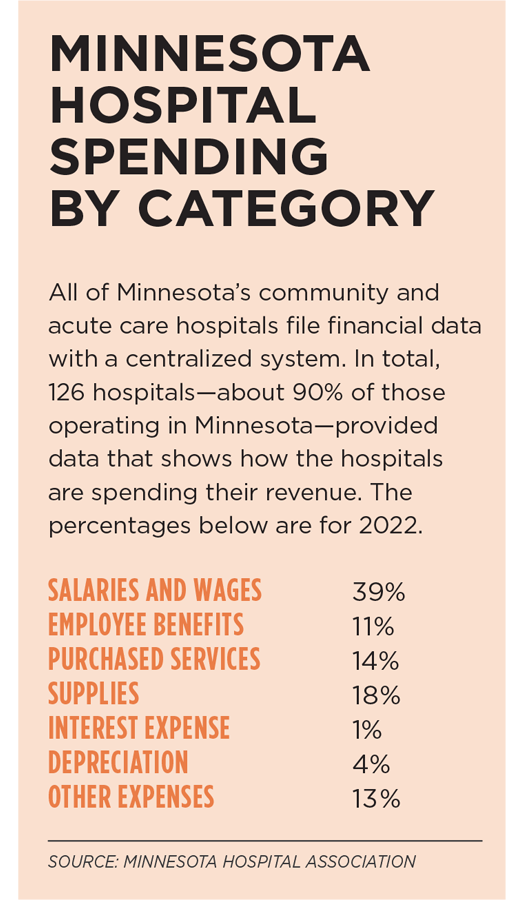
For the first half of 2023, Koranne says the hospital association’s survey shows that labor costs have increased by 7%, while supply and service costs jumped by 6%.
Koranne says he’s concerned that an increase in the proportion of Medicare and Medicaid patients could place health care facilities under greater financial pressure.
“Those programs continue to reimburse providers well below the actual cost of providing care, routinely underpaying an estimated 27% below cost for Medicaid, and 20% below cost for Medicare,” the hospital association said in November.
The federal Medicare program provides health insurance coverage for retirees and is supported by payroll taxes paid by employees and their employers. Medicaid provides health coverage for low-income Americans. Minnesota’s Medicaid program is called Medical Assistance
Based on the recent collection of health care data from 70 or so Minnesota hospitals, Koranne says the ratio of Minnesota patients covered by Medicare or Medicaid has risen from 62% in 2022 to 64% in 2023.
“Reimbursement [for medical services] is fixed and set by the government,” Koranne says. “We are not like Target, or a device maker, or a grocery store. We can’t raise our prices.”
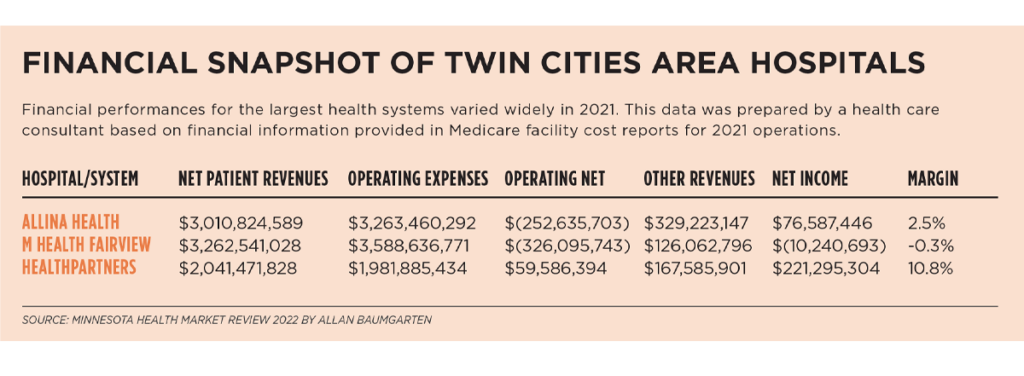
To respond to financial challenges, some health institutions are cutting programs and jobs. In August, Allina Health reported an operating loss of nearly $123 million for its second quarter. By late summer, it had cut more than 500 jobs.
In November, James Hereford, president and CEO of Fairview Health Services, reported a net operating loss of $315 million for 2022. He shared the financial data in an appearance before the Governor’s Task Force on Academic Health at the University of Minnesota. Fairview also cut hundreds of jobs last year.
Private vs. government insurance
Stephen Parente may be one of the few Minnesotans who understands the intricacies of health system business models and government health care reimbursement programs. He earned a Ph.D. in health finance and organization from Johns Hopkins University in 1995 and is a professor at the University of Minnesota’s Carlson School of Management.
He’s not as alarmed at the current state of affairs as Koranne is.
“Big picture, [the system] works well enough for the institutions that are operating right now,” Parente says. “That’s for sure nationwide. But it is the case that Medicare does pay less than commercial [insurers]. That’s been going on for decades. Medicaid pays even worse.”
Parente says private insurance subsidizes government underpayment with overpayment. “It is definitely true that they cross-subsidize their operations with some of the private pay from commercial and private insurers. But even within a hospital, there are certain specialties and areas that are basically going to give them more revenue and better revenue than others. The most revenue-generating part of a hospital today is orthopedic surgery,” he says. “It’s not just Medicare [patients]. It’s in demand for folks somewhere between 30 and 65 as they run more, exercise more, travel more, and break more things.”
The high volume of orthopedic surgery increases demand for adjacent services that include anesthesiology and radiology. “Anesthesiology, for obvious reasons—to put you under when you are going to get a hip replacement or a knee replacement,” Parente explains. “For radiology, they need to know where [in the patient’s body] they are going to be doing the surgery, so they’re going to need usually an MRI or a CAT scan.”
That “specialty combination” frequently subsidizes many other parts of a hospital’s operations that can be low margin, including pediatrics, OB-GYN, and sometimes psychiatry, Parente says.
The challenge of demographics
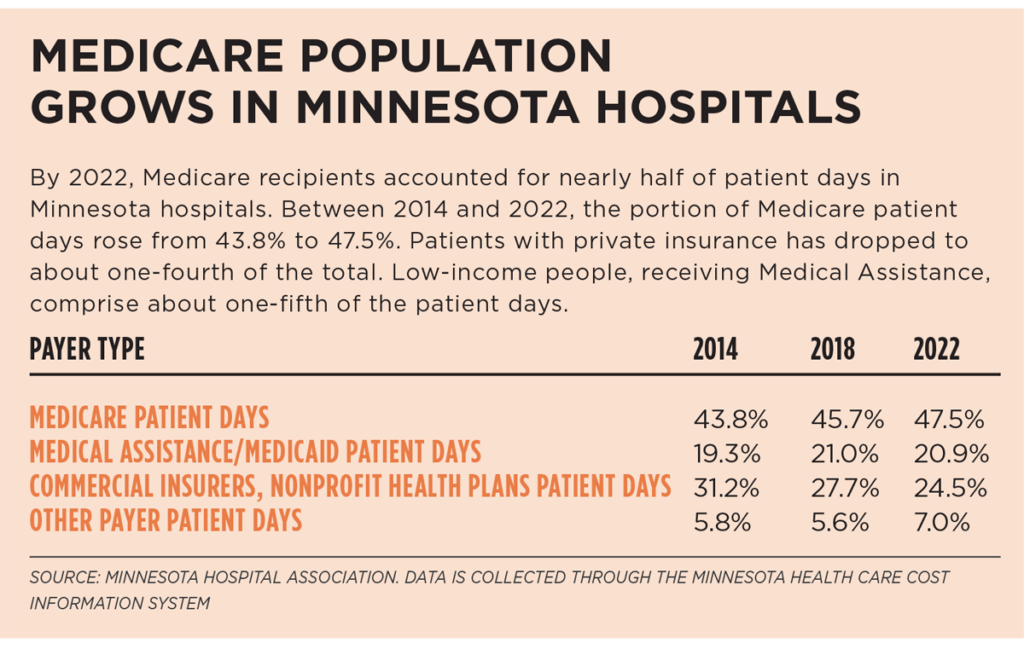
As many baby boomers enter Medicare coverage at age 65, that influx of older adults inevitably alters the patient mix at Minnesota hospitals and health systems.
Allan Baumgarten, a Minneapolis-based consultant on health care finance, does business analyses for clients such as health plans, providers, and government agencies. He’s seen a demographic shift over the last decade. In 2011, the percentage of in-patient days that were covered by Medicare or Medicaid in Twin Cities hospitals was 61%. That number had risen to 67.4% by 2021.
The total saw another boost in 2022, up to 69.4%. Baumgarten says the breakout was 41.7% of inpatient days covered by Medicare and 27.7% of inpatient days paid by Medicaid or the Children’s Health Insurance Program (CHIP).
“There is not agreement on this theory that Medicare and Medicaid are underpaying hospitals,” says Baumgarten, an attorney who has been producing the Minnesota Health Market Review annually since 1990. “It’s clear from data from Rand [Corp.] and others that the private payers are paying more,” he says. “But it’s not that clear that a hospital operating efficiently could not cover its costs and maybe even make money based only on Medicare rates—setting aside Medicaid.”
In his Minnesota Health Market Review 2022, he examines inpatient payer mix. In 2021, on an average day in Twin Cities hospitals, 73.3% of staffed inpatient beds were occupied.
“In 2021, Medicare, including Medicare Advantage plans and traditional Medicare, covered just under 40% of inpatient days, about the same as in the previous two years,” Baumgarten reported. “Medicare covered more than half of inpatient days at the HealthPartners hospitals, including 58.9% at Methodist Hospital. The Medicare share was lower at the Allina (44.1%) and Fairview hospitals (40.5%) and was only 3 2% at Hennepin Health.”
Like Baumgarten, Parente doubts that a higher concentration of Medicare patients in an aging society will jeopardize the durability of the health care revenue model. He points to the fact that many older adults are enrolled in Medicare Advantage plans, which are run by private insurers such as Humana and UnitedHealthcare.
“They have their own negotiated rates outside of Medicare of what they are paying for insurance,” Parente says. “People are choosing those plans, in part because they like some of the extra benefits they get for wellness and things like that that come along with them. They get pharmaceutical benefits as well.”
Medicare pays the insurance companies to cover people’s Medicare benefits when they have a Medicare Advantage plan.
Rising costs baked in
Over the past 30 years, on average, health spending in Minnesota increased by 5.8% each year, according to Baumgarten.
He notes that economists and financial experts see similarities between the higher education and health care sectors in their appetites for increased spending.
“The fact that there is revenue available from student loans has meant that universities have raised tuition rates and spending without much restraint,” Baumgarten says. “It’s correct to say that hospitals also will raise spending beyond what is covered by the rates paid by Medicare and Medicaid.” Some hospitals are undisciplined in their spending because they know they can turn to private payers for additional revenue, he says.
The federal Centers for Medicare & Medicaid Services released a report in mid-December that showed U.S. health care spending increased by 4.1% in 2022 to reach $4.5 trillion. Health care comprises 17.3% of the nation’s gross domestic product.
In some instances, Baumgarten says that Minnesota hospitals take costly paths that he believes could have been avoided.
“The hospitals, when it came to negotiating new nurses’ contracts, were willing to take a strike” in 2022, he says. “They incurred the expense of bringing in temporary nurses during those strikes rather than being more responsive to the demands of the bargaining units of the labor unions.” In 2022, nurses struck 15 Minnesota hospitals, which was classified as the largest private-sector nurses’ strike in U.S. history.
Role of investments
In 2022, Baumgarten says, stubborn inflation and higher labor costs reduced the net income of several hospitals and health systems. But he warns that it’s unwise to form any conclusions about health care finance by focusing on one year of performance.
“During the first year of Covid, there was a lot of angst or anxiety that hospitals would suffer mightily because they were seeing reduced revenues because they were suspending non-emergency surgeries,” he says. In addition, hospital leaders were worried in 2020 about the additional expense for treating Covid-19 patients.
“In 2019, and the year before that, the hospitals in Minnesota and in the other states that I study had very strong financial results, and so they came into 2020 with strong financial positions, which in a sense should be enough to weather a single down year,” Baumgarten says. Also, he says, hospitals were the recipients of provider relief programs from the federal government, so they could address Covid-related financial impacts to their business models.
He observes that Minnesota hospitals entered 2022 in good financial shape, and that some health systems benefited from ongoing consolidation within the industry. He also suggests a portion of hospital system losses may be unrelated to patient care costs.
“For many of the systems reporting reduced profits or even losses in 2022, that is mostly the result of unrealized losses on the value of their investment portfolios, which are priced to market at the end of each quarter and the end of the fiscal year,” he wrote in his market report. The national Health Affairs policy journal published an opinion piece in early 2023 in which the authors documented that 10 large, nonprofit health systems sustained major losses in the stock market in 2022.
The authors concluded: “Wall Street losses should not impact private payers’ and taxpayers’ payments to hospitals. Asking these constituents to foot the bill for hospitals’ investment losses not only lacks justification but will insulate hospitals from the consequences of their investment decisions.”
Stabilizing hospital finances
While Baumgarten and Parente take the long view when assessing the sustainability of the business model for Minnesota hospitals, Koranne emphasizes that some hospitals have real-time struggles, and he’s determined to press for state funding at the Minnesota Legislature.
In early 2024, Koranne says, hospitals are still housing patients who lack community placement options. “This discharge gridlock is causing problems for hospital and health system staffing, finances, and most importantly, making beds unavailable for new patients who need acute care.”
He also says hospitals have become engulfed in housing teens who actually need non-hospital care. “Emergency departments are boarding adolescents with mental health and violent tendencies because other care settings are overly reliant on hospital resources and 24/7/365 capacity,” he says. He emphasizes there’s a lack of psychiatric residential treatment facilities that would be in the best position to provide intensive mental health services for teens.
The Minnesota Hospital Association will be urging legislators to provide reimbursement to hospitals for the delayed patient discharges and emergency room boarding. It also will be asking for increases in Medical Assistance rates, financial support for mental health initiatives, and funding for strategies to expand the health care workforce.
Recently, 1 in 6 health care jobs were open in Minnesota. Koranne worries because health systems lack staff they need to care for patients and many students are bypassing health careers.
“The state has a responsibility to resuscitate the not-for-profit hospital and health care system,” Koranne says. “Once we get stabilization, then we can turn to innovation.”



