


Overuse of Medical Services Drives Up Costs for Everybody
My primary-care physician is a minimalist. Whatever malady prompts me to make an appointment and see him ends with the same medical advice: Lose weight and stop smoking. When I remind him I don’t smoke, he tells me to lose weight. He is loath to write a prescription or order a diagnostic test. So far, he’s been right. Whatever was bothering me goes away on its own, and I’m still here as I write this.
A spate of recent research suggests that my doctor is in the minority. Your workers are receiving millions of dollars’ worth of medical care that offers no clinical value. They’re also getting care from high-priced hospitals and doctors that could be provided for less without sacrificing quality and safety.
The next time you’re spending a few hours in your physician’s waiting room convinced you have a brain tumor, read the following studies and reports rather than a month-old Sports Illustrated:
- A study in the journal Health Affairs compared high-price physician practices with low-price physician practices using different outcome measures like patient experience, quality of care and spending (bit.ly/2oxnD4d). High-price practices charged an average of $84.45 for an office visit, or 36 percent more than low-price practices, which charged an average of $62.06 for an office visit. On most outcome measures, there were no statistically significant differences between high-price and low-price doctors. For example, the rate of preventive and screening services, hospitalizations and spending were similar, the study said.
-
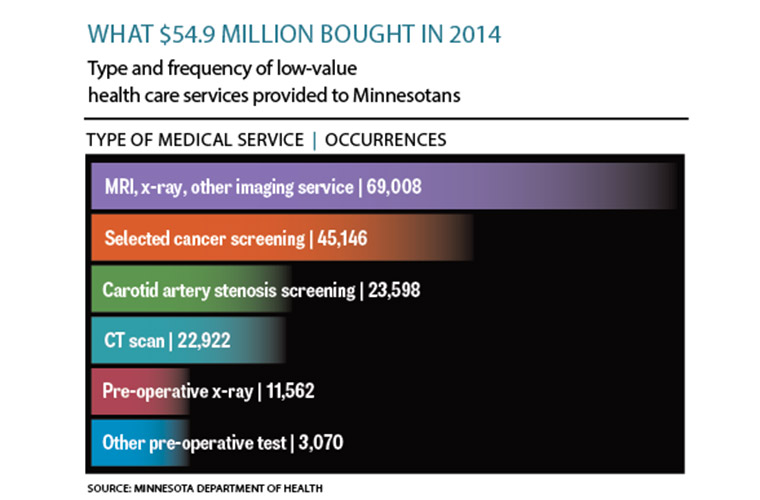
Closer to home, a report released by the Minnesota Department of Health said 175,306 low-value medical services were provided to state residents in 2014 at a cost of $54.9 million (bit.ly/2qBbegv).
Low-value services were one of 18 medical services that fell into three buckets: imaging procedures, screening procedures and pre-operative testing. They were defined as low-value—meaning they were largely unnecessary—by the Choosing Wisely campaign, the U.S. Preventive Services Task Force and the National Institute for Clinical Excellence in the United Kingdom. The report said commercial plans paid for the bulk of the low-value services—$29.2 million, or 53 percent, of the $54.9 million tab. Patients paid about $9.3 million out of pocket.
-
“Overuse of medical services is an increasingly recognized driver of poor-quality care and high cost,” said four doctors who stated the obvious in their article in the Journal of Hospital Medicine (bit.ly/2tQaj0M). The medical quartet published an action plan, or framework, that targets the underlying causes of too much medicine, including a culture of health care consumption.
I would recommend that employers and/or their health plans look at their framework and think about how they can apply it to their employees and enrollees to break the cycle of the overuse of unnecessary medical services.
They also should get involved in the Choosing Wisely campaign, a 5-year-old initiative that encourages providers and patients to limit medical services that meet four criteria (bit.ly/1dtkDI8). The services should be: supported by evidence; not duplicate other tests or procedures previously performed; free from harm; and truly necessary.
So if you get a headache from reading this column, do not go to the ER and have a CT scan. Take two aspirin and call my doctor in the morning; you’ll be fine. And lose some weight.
David Burda (twitter.com/@davidrburda, dburda@msp-c.com) is editorial director, health care strategies, for MSP-C, where he serves as the chief health care content strategist and health care subject matter expert.
Update
I might be right about provider-sponsored health plans but for the wrong reason. In our August 2016 column, we said employers should be skeptical of health plans owned by hospitals or health systems that also own physician practices (bit.ly/2uS4Sef). When one corporate entity controls all three pieces of the health care economic equation—outpatient care, inpatient care and how both are paid for—there’s less competition and more opportunity to manipulate prices.
Specifically, we said provider-sponsored health plans likely would offer lower premiums to attract more enrollees who then would use their affiliated hospitals and physicians for care. A 30-page report released by the Robert Wood Johnson Foundation said things aren’t working as planned (rwjf.ws/2tUi7y7). Prepared by Allan Baumgarten, a well-known health insurance analyst based in Minneapolis, the report said only four of 42 provider-sponsored health plans launched or acquired since 2010 turned a profit in 2015.
One of the 42—Gundersen Health Plan of Minnesota—lost $728,654 on about $5.3 million in revenue that year. “Few new plans have gained enough enrollees to achieve economies of scale in plan administration, to gain ability to manage risk, or to have an impact on competition and price in their local markets,” the report said. Those losses have to be made up somewhere, and the most likely somewhere is prices charged for inpatient and outpatient care. That’s why employers should be wary.



