The Promise and Pitfalls of Value-Based Care
On Wall Street, health executives love to talk about “value-based care.” Since 2011, the term has popped up in earnings calls 1,800 times, health news website Stat reported in early December.
The basic idea is to reimburse providers for actual health outcomes. In some cases, the concept transfers financial risks and rewards to providers based on performance benchmarks, which is why some value-based care arrangements are also referred to as downside or upside risk contracts. The goal, in either case, is to cut costs for patients and providers alike.
“Value-based care” has been bandied about locally, too. In August 2020, Eagan-based Blue Cross Blue Shield of Minnesota announced a six-year value-based care payment agreement with Allina Health. “We’ve lived in a volume-based health care world, where the profitability of sickness is greater than the profitability of wellness,” said Dr. Craig Samitt, then the CEO of Blue Cross Blue Shield of Minnesota. He held up the value-based agreement as a “positive example of what’s possible when health care plans and health care providers work collaboratively on shared challenges to improve the physical, mental, and financial health of our patients and members.”
As the agreement enters its fifth year, it remains to be seen whether those goals will be met in the long term in this specific case. Across the industry, agreements like these have long been held out as a balm for the many issues plaguing the American health system. Yet, even as health systems and insurers tout the benefits of value-based care, overall health outcomes in the U.S. still have not measurably improved. All the while, Americans still spend more on health care than any other high-income nation.
The shocking killing of UnitedHealthcare CEO Brian Thompson in New York City in early December, meanwhile, thrust many Americans’ long-simmering frustrations with health insurance back into the spotlight.
Though some health care industry observers see the potential of value-based care, many say that strictly value-based care arrangements remain stubbornly difficult to roll out on a wider basis rather than a piecemeal one, despite their popularity among executives and analysts. That’s due, in part, to a variety of factors: complex legal concerns about data-sharing among providers and payers, individual patients’ lifestyle choices, wider social determinants of health such as race and where you live, and many other factors that are similarly beyond providers’ control.
In some cases, too, there’s not always a firm agreement on the precise definition of value-based care.
“The value-based care landscape is just massive, and it could really mean almost anything,” says Ari Gottlieb, founder and principal of national health care consulting firm A2 Strategy Group. “As long as you’re paying somebody for something other than just the service they’re delivering, that’s all value-based care.”
Value, not volume
The push toward value-based care is not just a private-sector phenomenon; by 2030, the Centers for Medicare & Medicaid Services (CMS) aim to have 100% of Medicare beneficiaries in “accountable care relationships,” a specific type of value-based care arrangement.
There’s been some movement toward that goal, however ambitious. In 2023, 28.5% of all U.S. health care payments—through both commercial plans and federally funded ones like Medicare—flowed through downside risk contracts, according to the Health Care Payment Learning & Action Network, which tracks alternative payment models in the health care sector.
“Progress has been made, but it’s not as far along as any of us anticipated,” says Jean Abraham, professor at the University of Minnesota School of Public Health.
What many Americans can agree on is that we’re spending far too much on health care for widely varying outcomes. According to federal data, health care spending in the U.S. ticked up 7.5% in 2023, to $4.9 trillion. That equates t-o about $14,570 per person—about 17.6% of the nation’s gross domestic product.
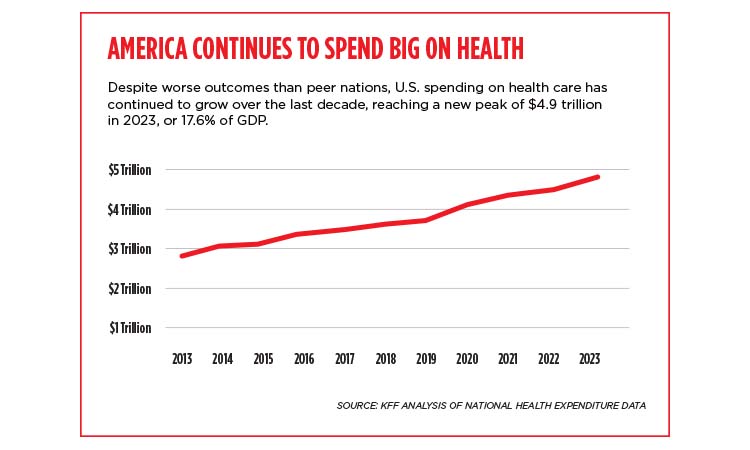
More money hasn’t led to better health outcomes, however. Among peer high-income nations, the U.S. has the “lowest life expectancy at birth, the highest death rates for avoidable or treatable conditions, the highest maternal and infant mortality, and among the highest suicide rates,” according to a January 2023 report by New York-based nonprofit Commonwealth Fund.
Though prospects for a U.S. universal health care system like those in the United Kingdom and Canada remain unlikely in the short term, the federal government remains the largest payer of health care in the country. That means that the direction of Medicaid and Medicare matters to both commercial payers and health care providers.
Gottlieb attributes some of the popularity of value-based care to the federal government’s goals, though it’s not immediately clear what direction CMS will take under Trump 2.0.
Read more from this issue

“The government has been pushing it” during the Biden administration, Gottlieb says.
Misaligned incentives
As some industry observers see it, one of the biggest barriers to implementing value-based care is the historical incentives of the American health system. For much of the modern era, providers have been incentivized for emergency care, says Dr. Tim Sielaff, executive fellow at the University of St. Thomas’ Opus College of Business and former chief medical officer at Allina Health.
“Miraculous things do happen in hospitals, tens of times every day,” Sielaff says, noting providers are “really good at rescue care.” But simply put, hospitals aren’t necessarily incentivized to reduce the number of patients occupying beds, for instance. Abandoning rescue care altogether, of course, isn’t really an option.
It’s a complicated problem that Sielaff describes as both “technical and adaptive.”
“In my work from being a doctor to being an executive, it’s the alignment of incentives across the continuum that is the principal complexity that hasn’t been solved to date,” Sielaff says. “I don’t see it being remarkably different from 20 years ago. The same issues are there.”
Then there’s the issue of patient choices coupled with social determinants of health—that is, the many nonmedical factors that affect someone’s health. A doctor can strongly advise a patient to quit smoking, but that doesn’t mean the patient will follow through. “We’re asking providers to do a lot because we know those things also matter for spending and utilization,” Abraham says.
Sielaff says that the advent of value-based care can be seen as an outgrowth of the movement toward HMOs (health maintenance organizations) in the 1990s. The basic idea is to limit coverage to providers who contract with an HMO. As any patient who’s had to look up “in-network providers” these days can attest, some tenets of that model remain today.
A bid to reduce waste
No one disputes that there is waste in the health system today—unnecessary tests or procedures, misdiagnoses, duplicated paperwork. The list goes on. “The problem with waste,” Sielaff says, “is that somebody is profiting from it.”
Value-based care evangelists say that their model, if implemented on a wider scale, could eliminate or reduce many of these factors.
“The problem with waste is that somebody is profiting from it.”
—Dr. Tim Sielaff, executive fellow, University of St. Thomas Opus College of Business; former chief medical officer, Allina Health
“We see value-based care as an opportunity to bend the cost curve lower for Minnesotans,” says Logan Nesse, president and CEO of the Minnesota Council of Health Plans, a trade group representing local nonprofit health plans, including Medica, UCare, and Blue Cross Blue Shield of Minnesota. “Multiple studies have recognized a surprisingly large proportion of expenditures—roughly a third—on health care services that are unnecessary or of minimal value for the patient. That adds costs, including out-of-pocket costs, for Minnesotans.”
He pointed to a 2017 report from the Minnesota Department of Health that cited diagnostic imaging for “uncomplicated headaches” as one of the most common and costliest low-value services.
“Historical payment arrangements based on volume of services have served as a financial incentive for doing them in the first place,” Nesse says. “Value-based care arrangements better align incentives to support efficient, cost-effective care.”

More data, more problems
Data sharing between providers and payers presents another major hurdle to implementing more value-based care arrangements. If payers don’t have all the data they need about lifestyles, for example, to determine a patient’s health outcomes, how can they know how much to reimburse providers? The Blue Cross-Allina partnership represents one potential answer, but it also illustrates how many potential solutions rest on a piecemeal basis between individual providers and payers.
“Providers themselves do not like the data to go much beyond their health systems,” says Stephen Parente, a professor at the University of Minnesota’s Carlson School of Management who studies health economics. “They don’t want it to free-flow into an insurance company or another third-party group to look at what’s going on there.”
The advent of electronic medical records might one day help smooth out the data flow issue, leading to more value-based care models, Parente says, but that will require a hefty amount of legal bargaining among all providers, payers, and patients.
Nesse with the Council of Health Plans argues that Minnesota might be in a better position than many other states to make that move. “Minnesota is recognized as having some of the best collaborations in the country between providers and insurers,” he says. “Integrated systems are presumably helpful for implementing arrangements, but the success outside of this model, as evidenced by the BCBS arrangement with Allina, shows it is not a necessity.”
Whatever the future of value-based care, most observers agree that it’s not going to happen quickly. Health care systems themselves don’t necessarily have a vested interest in transforming their operations. It could take another huge disruption like Covid to force change, some observers say.
“Markets can’t transform overnight. It’s probably a 10- to 20-year journey,” Gottlieb says.